
Last Modified: 06/21/2023
VIII. Live Evaluation Procedures
The following steps outline essential procedures to be followed during a tele-audiology session. Many tele-audiology procedures involve following standards for in-person evaluations.
Prepare the Patient Physical Environment and Infant State
As with any in-person audiolological service, the rooms at the spoke site and hub site for a tele-audiology session should be set up in a welcoming and professional way.
- Ensure privacy in both the patient location (spoke) and the specialist (hub) location. The American Telemedicine Association suggests “efforts should be made to ensure privacy so clinical discussion cannot be overheard by others outside of both the patient room and the specialist room where the service is provided. If other people are in either the patient or the professional’s room, both the professional and patient shall be made aware of the other person and agree to their presence.” (ATA, Practice Guidelines).
- “Both professional and patient should maximize clarity and visibility of the person at the other end of the video services. Cameras should be on a secure, stable platform to avoid wobbling and shaking during the videoconferencing session. To the extent possible, the patient camera should be placed so that the infant’s head will be clearly visible to the other person.” (ATA, Practice Guidelines).
- The test environment should be conducive to sleep. A dimly lit, quiet room, free from visual distractions and other disturbances is critical. A portable, dimmable light source may be helpful. A battery powered LED light will also reduce the possibility of electromagnetic test interference from fluorescent lighting.
- Minimize the number of people at the spoke site. Where possible, restrict entry to one parent or caregiver and the spoke site technician.
- Wherever possible, a spoke site selection visit should be made by the audiologist to ensure that the test environment is appropriate. A pilot ABR test without an infant should be conducted to ensure that ambient noise is appropriate and that electromagnetic noise will not interfere with the ABR.
- Cell phones should be turned off for all participants in the evaluation process. Caregivers can be provided ample time for communication with family members present regarding the process during test breaks or after the session is complete.
Ambient Noise
Due to the nature of tele-audiology, an audiometric test room may not be available at the spoke site. Although tone burst ABR with insert earphones tends to be resistant to ambient noise, care must still be taken to ensure the test environment is appropriate and that ambient noise will not lead to error in test results. Spoke site rooms should be located in areas where surrounding noise is minimal. When possible, ambient noise levels should be checked by the audiologist during a spoke site selection visit. If this is not possible, ambient noise should be verified by the audiologist prior to testing. This can be done with a sound level meter or a smartphone app that has been approved by the audiologist. The test can be conducted by the spoke site technician under the instruction of the audiologist.
Infant ABR testing under most EHDI protocols does not occur below 25 dB eHL. Evidence indicates that occlusion effects are clinically insignificant in infants (Small et al. 2007); therefore, it is not necessary to remove insert earphones when testing bone conduction. The chart below indicates the maximum permissible ambient noise levels (MPANL) when testing to 25 dB eHL according to ANSI S3.1.
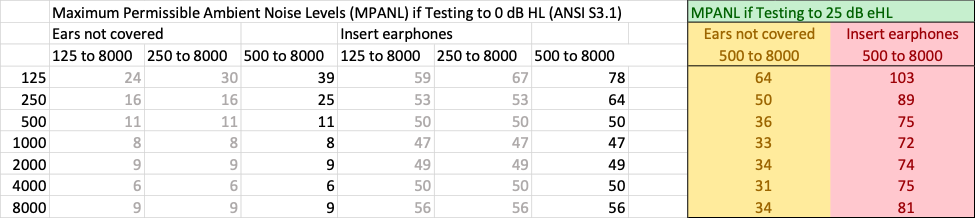
Image used with permission from Scollie, S, Western University, London Ontario
Prepare the Infant
The Ontario Infant Hearing Program ‘Protocol for Auditory Brainstem Response-Based Audiological Assessment, v2018.01 (the guiding document for the Ontario IHP tele-audiology protocol) describes the Pre-Test Baby State: “Typically it is desired that the baby arrive for the appointment hungry and tired, though not overtired. After cursory otoscopy and ABR electrode attachment, that baby can be fed and prepared for sleep. It usually follows that the baby should be neither fed nor allowed to sleep within an hour prior to the appointment.” The family or caregivers should be made to clearly understand that a successful test depends on their following pretest instruction carefully. Brief, clear, and strongly worded messaging to the family is critical to avoid wasting appointment times.
Avoid eye contact, engaging facial expressions, and verbal communication with the infant. Over-engagement with the infant is likely to preclude sleep. Physical restriction such as swaddling along with gently rhythmic movement and soothing, simple sounds are helpful. Swaddling the infant has been shown to be a key factor in promoting sleep (Nelson, 2015). Once the baby has been prepared for testing (swaddled, electrodes and insert earphones in place), breast or bottle feeding may be helpful to promote sleep. Care must be taken to position the infant to avoid issues with gas that may awaken the baby during the test.
Confirm the Identities of All Present
The name and credentials of the diagnosing audiologist, the assistant at the patient site, and the name of the patient shall be verified at the start of the live session. This can be initiated by the assistant at the patient site or by the audiologist. In addition, ATA has provided the following rules to be followed (ATA, Practice Guidelines):

- All individuals present/entering each site must be introduced to the parent/caregiver.
- All individuals entering the patient site should be introduced to the specialist.
- When an individual leaves either site this should be communicated to each site.
- Parent/caregiver must agree to all individuals entering either room. It is possible for parents/caregivers not to be aware that someone has entered the room because they cannot see or hear that person, so it is the responsibility of the specialists to announce anyone else in the room at either site.
- All observers who are at the specialist site must be invited in the room after the parent/caregiver has given permission. They should not be in the room when the call is connected because this does not allow for permission.
The HIPAA protocols employed by the hub site also extend to the spoke site.
Confirm Roles During the Diagnostic Process
The parent/caregiver of the infant being assessed should receive clear information about the roles of the assistant and the diagnosing audiologist. This is important to ensure that the parent/caregiver understands that the diagnosing audiologist is the provider who is providing the direct service and the provider with whom the parent/caregiver is to direct communications regarding the procedures, results, and follow up.
Modified Evaluation
While all assessment procedures that use a remotely controlled PC are easily performed using tele-audiology, some accommodations are likely in conducting a full remote audiological assessment. Facilities using tele-audiology should ensure that a consistent and agreed upon tele-audiology protocol is in place. Everyone at the hub and spoke sites must be aware of expectations and limitations because protocols and goals may vary from site to site. Some programs support the goal of a modified evaluation while others want the services provided to be the equivalent of what would be provided in a pediatric audiology facility. The critical piece of any infant hearing assessment is to safely and efficiently determine hearing status. This is best achieved through the ABR test. Other tests in the assessment battery, such as OAE, tympanometry, and acoustic reflex measures, may be considered as discretionary and only included in the assessment process if ABR results dictate by some programs, while others may desire that a complete test battery be completed.

- The audiologist will direct the spoke site technician in cursory video otoscopy. The objective of otoscopy in remote ABR assessment is to ensure that there are no contraindications to the use of insert earphones. It is not necessary to ascertain the condition of the tympanic membrane at this time. Therefore, a very cursory inspection is appropriate.
- The audiologist will direct the spoke site technician to place appropriate probes in the infant’s ears as the test session progresses. This may include insert earphone transducers for Auditory Brainstem Response (ABR), a probe for Otoacoustic Emissions (OAEs) or a probe for immittance measures.
- The audiologist directs the spoke site technician to attach the electrodes to the infant. Recording electrodes are used for diagnostic ABR assessment. Electrode impedances (or contact to the skin) can have significant effects on successful testing and is an important task for the assistant. The audiologist will need to be sure that the appropriate impedance values are met.
- Immittance measures may be difficult to obtain remotely, as maintaining an hermetic seal in the ear canal may be challenging for a remote site technician. Where appropriate within the pertinent protocol, immittance measures should be considered as an adjunct or discretionary test in remote ABR assessment. Immittance measures are generally not necessary where normal hearing has been indicated by ABR. If abnormal ABR results are obtained, immittance measures may be obtained at a later, in-person, follow up appointment.
Review Materials for Technician Prior to Evaluation
Wisconsin video clips of tele-audiology session
References
- Nelson, A.M. (2017). Risks and Benefits of Swaddling Healthy Infants: An Integrative Review. American Journal of Maternal Child Nursing, 42(4); 216-225.
- Ontario Infant Hearing Program. (2019). Protocol for Audiological Surveillance of Children At Risk for Permanent Hearing Loss. Version 2019.01. https://www.uwo.ca/nca/pdfs/clinical_protocols/IHP%20Surveillance%20Protocol_2019.01_Final_July_2019.pdf [PDF]